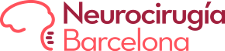
Astrocytomas form part of the group of gliomas (glial tumours), they are primary brain tumours, that is, tumours that originate in cells that form part of the normal brain structure. Within the group of glial tumours, astrocytomas represent the most frequent tumours.
They may be located at any point of the neural axis (brain and spinal cord) even though they are especially common at a level of the cerebral hemispheres. Gliomas of the optic nerve, thalamic astrocytomas and astrocytomas of the brain stem and spinal cord are worth special mention as they present particular characteristics regarding their location and histology and so personalised treatment is recommended for this type of lesion.
The symptomatology presented by these tumours is quite similar to other cerebral lesions, headache, vomiting, gait disorders, seizures, etc. the symptoms may be brought about by invasion of the tumour into area responsible for these functions, by the oedema (swelling) these lesions produce in the brain or by the simple compressive effect they have on healthy surrounding tissue.
Astrocytomas make up a heterogeneous group, classified by the WHO in four degrees (1993) based on their histological characteristics:
- Astrocytoma grade I (pilocytic astrocytoma): especially common among children. Presenting very good prognosis, as complete resection implies cure in the immense majority of cases.
- Astrocytoma grade II, or diffuse astrocytoma: This group is comprised of different sub-groups with particular characteristics. It is an infiltrating tumour with a tendency to evolve into lesions with a more aggressive histology.
- Astrocytoma grade III or anaplastic astrocytoma: This tumour is equally invasive, although its histological characteristics give it a worse prognosis than the previous groups, it may evolve into glioblastoma multiforme.
- Astrocytoma grade IV or Glioblastoma multiforme: The most aggressive and at the same time most common of all astrocytomas.
The treatment of choice for all resectable tumours will be surgery, associated with concomitant radiotherapy and chemotherapy treatment in some cases, especially the most aggressive ones.
On a medullary level they are infiltrating tumours with poorly defined margins, and so the treatment of choice in this location will be biopsy.
Over the last few years different lines of treatment have appeared, including immunotherapy, vaccines, etc., even though all of them are still in the evaluation phase.