Cranial deformities are a common reason for consultations during the first few months of life. The causes are varied and may be related to mechanical, intrauterine, intrapartum or postural factors secondary to the supine decubitus (face up) position usually recommended for nursing infants to reduce the risk of cot death. However, in certain cases, the cranial deformity has an organic cause and is due to early closure of the cranial sutures. In these cases the term is craniosynostosis.
Craniosynostosis prevents normal growth of the cranium and produce a deformity that becomes more evident with growth. The implications are basically aesthetic although, in some cases, there may be a functional repercussion. For this reason a paediatric neurosurgeon should evaluate the cranial deformity, establish the protocol for diagnosis imaging considered most convenient and explain the most suitable therapeutic possibilities for each case.
It is important to note that not all cranial deformities are candidates for surgical treatment but whenever this is the case, the treatment should be performed at a specific moment of development to reduce risks and favour results. This means it is extremely important to make an early diagnosis. What we should know about cranial deformities:
- The majority of cranial deformities present at birth are associated with intrauterine conditions (multiple pregnancies) or intrapartum shaping (forceps, suction cup) and improve spontaneously during the first 6 weeks of life.
- Cranial deformities that develop postnatally are mainly related to congenital torticollis or with the supine position during sleep. The recommendation of the American Academy of Pediatrics (AAP) in 1992, regarding placing infants in the supine position when sleeping “Back to Sleep”, or the measures for prevention of the sudden infant death syndrome (SIDS), have favoured the appearance of cranial deformities. The invariable supine position with the head turned the same side since birth causes plagiocephaly and always face upward causes brachycephaly.
- Posterior positional plagiocephaly is defined as a deformity consisting of uni or bilateral occipital flattening, with of the Ipsilateral frontal bossing, sometimes the cranium is not closed and larger in size, and contralateral occipital bulging. There are cases with a frontal bulge, protrusion of the cheek bone and deviation of the ipsilateral lower jaw. Treatment is postural and only severe cases may require a cranial orthosis (helmet).
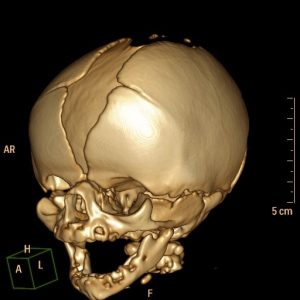
- Craniosynostosis consists of early closure of certain sutures. Depending on the suture, this may produce different types of deformities:
- Scaphocephaly: elongated head with frontal and occipital protrusion
- Plagiocephaly: asymmetric deformity involving facial scoliosis and contralateral bulging of the forehead
- Brachycephaly: cranium with a smaller antero-posterior diameter. Associated with microcephaly and may cause problems with psychomotor development
- Trigonocephaly: triangular forehead with a bony crest in the Center
In the majority of cases these deformities require early surgical correction. The paediatric neurosurgeon should assess each particular case and indicate the most appropriate technique for each patient as well as best moment for applying treatment. In the majority of the cases surgery will consist of reopening the closed suture associated with different surgical techniques that enable remodelling cranial morphology.