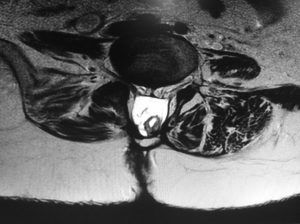
One of the most frequent congenital malformations are those derived from defects in neural tube closure and cover a wide range of presentations usually called spina bifida or spinal dysraphism. Characteristically a first distinction is made between open and occulta spina bifida.

- Closed spinal dysraphy is the mildest form and the skin is unscathed or presents so-called “cutaneous stigmata”. It is associated with malformation of one or more vertebrae (incomplete closure) and involves soft tissues (fat, muscle, meninges, etc.) to a various extent. They are not always symptomatic at birth but the clinical signs evolve during growth causing neurological symptoms associated with anchored marrow. It requires careful and multidisciplinary follow-up and, in some cases, surgical “untethering” is recommended.
- Open spinal dysraphy is evident at birth and consists of larger defects, with partial or incomplete skin coverage and extrusion of the spinal contents (meninges, medulla, nerve roots). It requires early surgical closure and follow-up of complications associated with the secondary spinal cord tethering. The most common neurological affectations are:
- Motor disorders.
- Sensitivity disorders.
- Sphincteric disorders.
- Deformities of the lower extremities.
- Other disorders (Chiari, hydrocephalus, etc.)
It is important to note that many children suffering from spina bifida lead a totally normal life with very few restrictions compared to their companions. Nevertheless the risk of decompensation during growth requires strict multidisciplinary control.