Pineal tumours are lesions originating in the pineal gland. These lesions are most frequent in infancy (3-8% of brain tumours in children) than among adults.
Clinical signs
 Due to their location they may cause obstruction of the cerebrospinal fluid drainage and produce hydrocephalus. Other symptoms are Parinaud’s syndrome and early puberty in children.
Due to their location they may cause obstruction of the cerebrospinal fluid drainage and produce hydrocephalus. Other symptoms are Parinaud’s syndrome and early puberty in children.
Diagnostic tests
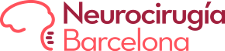
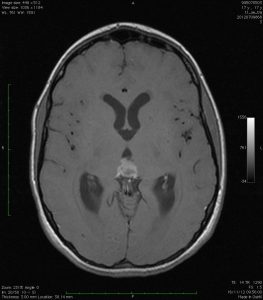
These tumours release markers into the blood stream and cerebrospinal fluid although they are insufficient for a definite diagnosis in the majority of cases. Tumour markers: chorionic gonadotropin, alpha-fetoprotein and carcinoembryonic antigen. Magnetic resonance imaging is essential for correct definition of the tumour and its anatomical connections.
Treatment
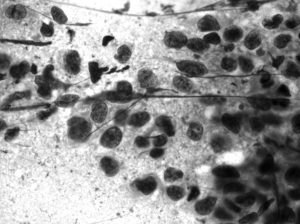
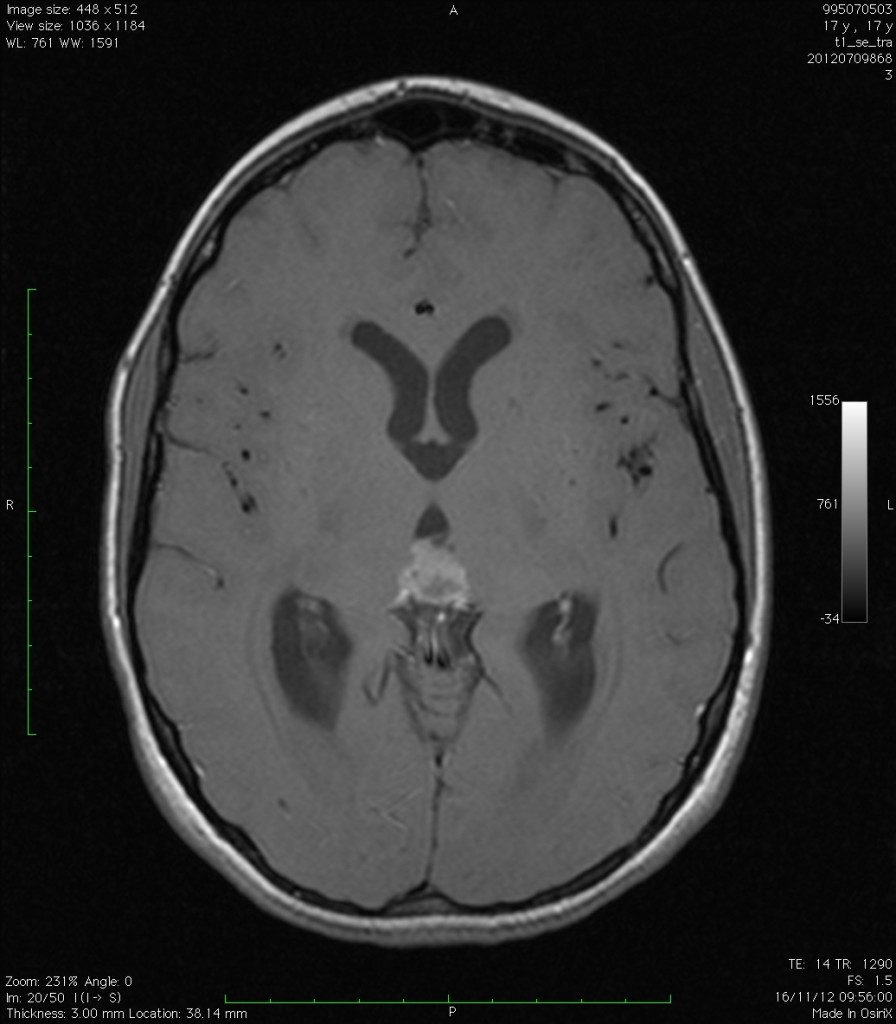
It is of vital importance to have experience with this type of tumours and know how to relate radiological findings with tumour markers to distinguish between the different tumour subtypes. Surgical and adjuvant treatment will vary depending on the tumour subtype:
- Germinomas: the role of surgery is merely diagnostic, no vast exeresis is required. The treatment of choice is radiotherapy and sometimes chemotherapy.
- Pineocytomas: the treatment of choice is complete surgical resection. If resection is partial radiotherapy is required.
- Pinealoblastomas: treatment is a combination of surgery, chemotherapy and craniospinal irradiation with local overdose.
- Teratomas:surgery is the treatment of choice. The treatment of choice for the hydrocephalus associated with these lesions, will be endoscopic third ventriculostomy, endoscopic techniques (minimally invasive) to resolve the obstruction without any need for placement of a shunt. Endoscopic techniques can also be used to obtain a biopsy and analyse the pathological anatomy of the tumour without any need for open surgery.